Office-based, no radiation
Ultrasound-Guided Injections
For nerves, bursae, and peripheral joints, ultrasound is the right imaging tool. I see the anatomy and the needle in real time — no radiation, no contrast dye, and no surgery center required. Most of these I do in the office. Below is what I treat, what to expect, and what the visit looks like.
What ultrasound lets me do
See the anatomy and the needle, in real time, with no radiation
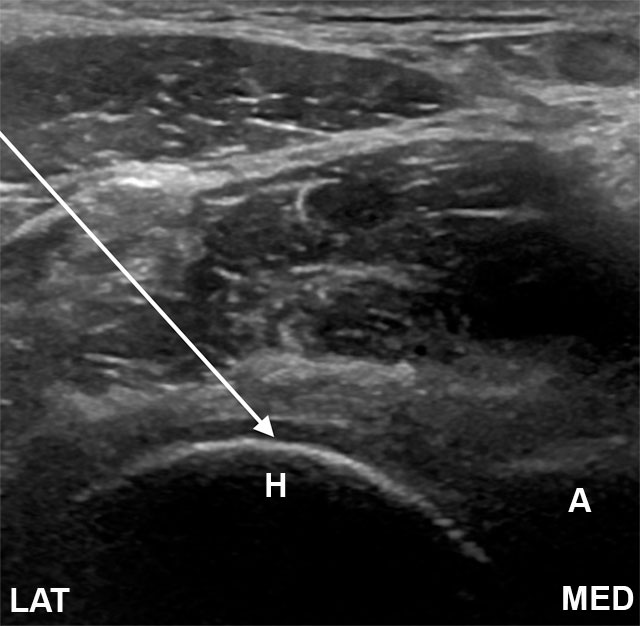
Ultrasound shows me what an X-ray can't: nerves, tendons, blood vessels, joint capsules, and the medication itself spreading where I want it to go. For most peripheral procedures, it's the right tool.
I hold the transducer with one hand and the needle with the other. I watch both on the screen the entire time. When the needle reaches the right structure, I deliver the medication and watch it spread — confirmation in real time that I'm in exactly the right space. No radiation, no contrast dye, no surgery center, no fasting, no IV.
What I treat falls into three categories: nerves (nerve blocks for specific peripheral nerves), bursae (the fluid-filled cushions that inflame and cause focal pain), and joints(the smaller peripheral joints where ultrasound shows me the capsule and the medication spread better than fluoroscopy would). Below are the targets I see most often — there are others. If yours isn't listed, ask.
Section 1
Nerve blocks
When pain comes from a specific peripheral nerve, I can numb that nerve directly. The first hour after the block is diagnostic — significant relief confirms that the nerve was the source. Sometimes the block alone gives durable relief; sometimes it tells me the right nerve to target with a longer-lasting procedure later.
Suprascapular nerve block
I numb (and sometimes long-act) the nerve that supplies most of the back of your shoulder joint and rotator cuff.
Where this fits: Stubborn shoulder pain after rotator cuff surgery, frozen shoulder (adhesive capsulitis), or chronic shoulder arthritis when steroid injections aren't enough. Often dramatic immediate relief that's also diagnostic.
Lateral femoral cutaneous nerve block
I target the small sensory nerve that runs over the front and outer thigh, giving relief for meralgia paresthetica.
Where this fits: Numbness, burning, or 'a wallet feeling' over the outer thigh — often from compression at the inguinal ligament after weight gain, pregnancy, tight belts, or a long surgery in lithotomy position.
Intercostal nerve block
I numb one or more of the nerves that run along the underside of each rib.
Where this fits: Focal chest-wall pain after rib trauma, surgery (thoracotomy, mastectomy), or shingles. Especially useful when post-herpetic neuralgia is in a single dermatome.
Other peripheral nerves I block under ultrasound include genicular nerves around the knee, occipital nerves at the base of the skull, ilioinguinal, pudendal, and others — depending on where your pain is.
Section 2
Bursa injections
Bursae are small fluid-filled cushions that sit between bones, tendons, and skin to reduce friction. When they inflame, they cause focal, often deep pain that's frequently mistaken for arthritis. Ultrasound shows me which bursa is inflamed and lets me inject it precisely without hitting the nearby tendon.
Greater trochanteric bursa
I inject the deep bursa over the bony point on the outside of your hip (greater trochanter).
Where this fits: Sharp pain on the outside of your hip that's worse lying on that side, walking up stairs, or after standing too long. Often misdiagnosed as 'hip arthritis' when it's actually trochanteric bursitis or gluteal tendinopathy.
Subacromial bursa
I inject the bursa that sits between your rotator cuff and the bony arch of your shoulder (acromion).
Where this fits: Painful arc with overhead reaching, night pain, and a 'pinching' feeling lifting your arm. Common in rotator cuff impingement and bursitis.
Scapulothoracic bursa
I inject the bursae between your shoulder blade and the back of your rib cage.
Where this fits: Snapping or grinding under your shoulder blade with movement, a deep ache when reaching across your body, often in patients with poor scapular mechanics or after thoracic surgery.
Other bursae I treat depending on your case: olecranon (elbow), prepatellar / pes anserine (knee), retrocalcaneal (heel). If you have focal pain that worsens with pressure or specific movement, ask me.
Section 3
Peripheral joint injections
For peripheral joints — outside the spine — ultrasound usually beats X-ray. I see the joint capsule, the surrounding soft tissues, and the medication spreading inside the joint, all in real time.
Hip joint injection
I inject anti-inflammatory medication directly into the hip joint capsule under live ultrasound.
Where this fits: Hip arthritis, labral pain, post-surgical hip pain, and avascular necrosis. The first hour after injection is also diagnostic — dramatic relief confirms the joint as the source.
Read the full guideShoulder joint (glenohumeral) injection
I inject the main shoulder ball-and-socket joint under live ultrasound.
Where this fits: Shoulder arthritis, frozen shoulder (especially when paired with hydrodilation), and post-traumatic shoulder pain. Good first interventional step before any surgical conversation.
Talonavicular joint injection
I inject the small joint on the inside of your midfoot, where the talus meets the navicular bone.
Where this fits: Midfoot pain that's worse with walking on uneven ground, after old foot fractures, in early arthritis, or after a missed Lisfranc-type injury. Easy to overlook on imaging — easy to confirm with a precise injection.
I also do ultrasound-guided injections of the AC (acromioclavicular) joint, sternoclavicular, elbow, wrist, ankle, and small joints of the hand and foot. The pattern is consistent — see the joint, place the medication exactly where it needs to go.
Honest expectations
What to expect across all of these
What this can do for you
- Targeted relief at the actual source — nerve, bursa, or joint — with real-time imaging confirmation.
- First hour is diagnostic — dramatic relief from the local anesthetic confirms we're treating the right structure.
- No radiation, no contrast dye, no IV, no fasting, no driver required for most.
- Office-based — you walk in, we do the procedure, you walk out. Usually 30–45 minutes total visit.
- Lets you participate in physical therapy and rehab without pain limiting your effort.
Risks I'll be honest about
Most are uncommon and most are short-lived.
- Soreness at the injection site for a day or two(common)
- Brief bump in blood sugar — important if you have diabetes(common in diabetics)
- A 'flare' — temporary worsening of pain in the first 24–48 hours(occasional)
- Skin pigment lightening at the injection site (with steroid)(rare)
- Vasovagal response (lightheadedness, brief drop in blood pressure)(occasional)
- Bleeding into a joint or bursa, especially if you're on blood thinners(rare)
- Infection — septic arthritis if a joint, bursitis if a bursa(very rare)
- Allergic reaction to the steroid or numbing medication(rare)
Before your visit
How to get ready
Office-based ultrasound injections are simpler than spine procedures at the surgery center, but a few things still matter.
Bring a driver
Eating and drinking before
Take your morning medications
Blood thinners — talk to me first
- • Aspirin (81 mg) — usually OK to continue. I'll tell you if I want it held.
- • Plavix (clopidogrel) — typically held 5–7 days before
- • Eliquis (apixaban) — typically held 24–48 hours before
- • Xarelto (rivaroxaban) — typically held 24–48 hours before
- • Pradaxa (dabigatran) — typically held 24–72 hours, depending on kidney function
- • Warfarin (Coumadin) — typically held until INR is below 1.5
- • Lovenox (enoxaparin) — typically held 12–24 hours
Tell me about your allergies
What to wear
After
Recovery and what to watch for
First few hours
The numbing medication may give you dramatic immediate relief. Enjoy it — it's diagnostic. Drive home, light activity for the rest of the day.
Hours 4–48
Numbing wears off, steroid hasn't fully kicked in yet. Some patients have a 'flare' (temporary worsening). Ice, Tylenol, NSAIDs as you'd normally use them. This is expected and self-resolves.
Days 3–7
The steroid starts working. Most patients notice meaningful improvement during this window. Resume normal activity, including physical therapy.
Weeks 2–6
Peak benefit. Use this window for the strengthening / rehab work that produces durable relief.
When to call me right away
Severe new weakness in your arms or legs
If a limb feels significantly weaker than before — trouble lifting it, dragging a foot, dropping things — that needs attention now.
Loss of bladder or bowel control
Sudden trouble holding it or sudden trouble going. Rare, but a true emergency. Go to the ER, then call me.
Fever above 101°F (38.3°C)
A fever in the days after the procedure, especially with chills, can mean infection.
Spreading redness, warmth, or drainage at the injection site
Some bruising and tenderness is normal. Pus, increasing redness expanding outward, or yellow drainage is not.
Severe new pain that's worse than before
Brief soreness for a few days is expected. Sharp, severe new pain different from your usual is not.
For anything that worries you, call my office. I'd much rather hear from you and tell you it's fine than have you wait at home wondering. For loss of bladder/bowel control or anything that feels like a true emergency, go to the nearest ER — then call me.
The questions I get most
Frequently asked
Will I be put to sleep?
Why ultrasound and not X-ray for these?
Do I need someone to drive me?
How fast will I feel better?
How long does the relief last?
Can I have it again?
What if it doesn't work?
I have a target that's not on this page — can you still inject it?
Have Questions?
If you'd like to learn more about your treatment options or have a question for Dr. Patibanda, reach out.
Contact Dr. Patibanda