Ultrasound-guided joint injection
Ultrasound-Guided Hip Injection
If your hip pain is coming from inside the joint — arthritis, a labral tear, or capsular inflammation — a precise injection of medication into the joint can give you real relief. I use ultrasound, which means no radiation and no contrast dye. Here's exactly what happens.
What I'm doing
Calming the joint that's been quietly wrecking your day
Your hip is a deep ball-and-socket joint sitting under layers of muscle and fat. Hitting the joint space precisely from the outside isn't something I can do reliably by feel alone — and a missed injection is a wasted injection.
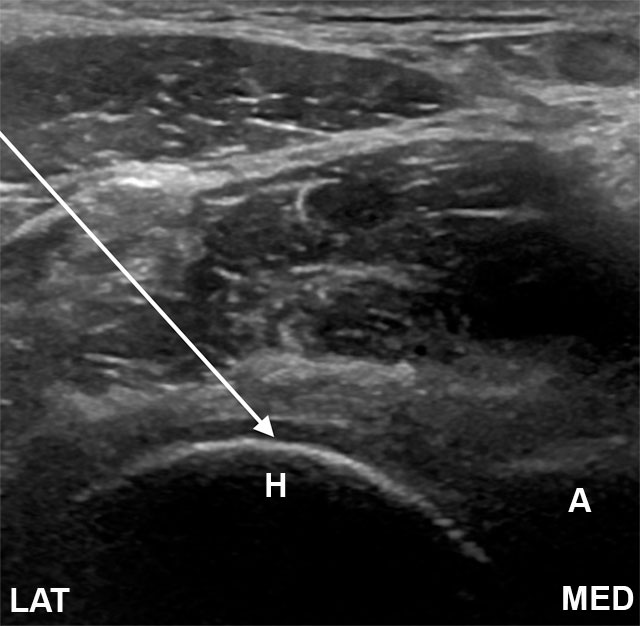
That's why I use ultrasound. Ultrasound shows me the joint capsule, the femoral head, the surrounding blood vessels, and — once I'm in — the medication spreading exactly where I want it to go. I can see all of this in real time, on the screen next to me, with no radiation and no contrast dye.
I deliver a corticosteroid (anti-inflammatory) often combined with a local numbing medication. The steroid quiets the inflammation in the joint. The numbing medication gives you immediate diagnostic information — if your pain drops dramatically within an hour, we've confirmed the joint was the source. If you have specific reasons to avoid steroids (well-controlled diabetes is fine, but uncontrolled diabetes is a discussion), we can talk about other options like hyaluronic acid or PRP at a different visit.
One thing I want to be clear about: this isn't fixing the underlying arthritis or labral damage. It's reducing inflammation so the joint hurts less while you build the strength and conditioning that produces durable relief. For some patients, an injection plus PT buys years of comfort. For others with end-stage arthritis, it's a bridge to talking with an orthopedic surgeon about replacement.

Honest expectations
What this can do — and what it can't
A well-placed hip injection can be remarkable. It can also be modest. Here's the realistic picture.
What this can do for you
- Targets the actual source of your pain — the joint itself, not a body-wide painkiller.
- Gives me diagnostic information: dramatic pain relief in the first hour confirms the joint was the source.
- No radiation. No contrast dye. Done in the office, not at a surgery center.
- Lets you participate in physical therapy and the strengthening work that produces lasting improvement.
- Can postpone or avoid hip replacement when symptoms are mild-to-moderate.
Risks I'll be honest about
Most are uncommon and most are short-lived.
- Soreness at the injection site for a day or two(common)
- A short bump in blood sugar — important if you have diabetes(common in diabetics)
- A 'flare' — temporary worsening of joint pain in the first 24–48 hours(occasional)
- Skin pigment lightening at the injection site(rare)
- Infection of the joint (called septic arthritis)(very rare)
- Bleeding into the joint, especially if you're on blood thinners(rare)
- Allergic reaction to the steroid or numbing medication(rare)
Other options
Things we could try instead, or alongside
An injection is rarely a complete plan on its own. The right approach usually combines a few of these depending on what's driving your pain and how advanced the joint changes are.
Physical therapy
Targeted hip and core strengthening — especially the gluteal stabilizers — can dramatically reduce hip pain over weeks.
Where this fits: Always part of the long-term plan. An injection often makes PT possible.
Hyaluronic acid (viscosupplementation)
A gel-like injection that lubricates the joint. Different mechanism than a steroid, sometimes useful when steroids aren't a fit.
Where this fits: Mild-to-moderate hip arthritis, especially if you've responded poorly to steroids.
PRP (platelet-rich plasma)
Concentrated growth factors from your own blood, injected into the joint. Limited but growing evidence for hip osteoarthritis.
Where this fits: Younger or active patients who want to avoid steroids and have realistic expectations.
Anti-inflammatory medications
NSAIDs (ibuprofen, naproxen, meloxicam) and Tylenol can reduce day-to-day pain.
Where this fits: First-line for mild symptoms, when your kidneys and stomach tolerate them.
Weight management and activity modification
Every pound off your body is roughly four pounds off your hip joint with each step. The math matters.
Where this fits: Almost always part of the picture for hip pain — even small changes shift the trajectory.
Orthopedic surgery consultation
If imaging shows end-stage arthritis or a structural problem that won't respond to injections, total hip replacement is a remarkably good operation.
Where this fits: When conservative care has failed, when pain is changing your life, when imaging clearly explains it.
Before your visit
How to get ready
The pre-procedure rules for an office-based ultrasound injection are simpler than for a spine procedure at the surgery center. Read all of these — a few still matter.
Bring a driver
Eating and drinking before
Take your morning medications
Blood thinners — talk to me first
- • Aspirin (81 mg) — usually OK to continue. I'll tell you if I want it held.
- • Plavix (clopidogrel) — typically held 5–7 days before
- • Eliquis (apixaban) — typically held 24–48 hours before
- • Xarelto (rivaroxaban) — typically held 24–48 hours before
- • Pradaxa (dabigatran) — typically held 24–72 hours, depending on kidney function
- • Warfarin (Coumadin) — typically held until INR is below 1.5
- • Lovenox (enoxaparin) — typically held 12–24 hours
Tell me about your allergies
What to wear
The visit
Step by step, what actually happens
The whole appointment is usually 30–45 minutes door-to-door. The injection itself takes 10 minutes once we're set up.
- 1
Arrival
Come into the office, check in at the front desk. No fasting, no IV, no gown for most patients — you'll roll up your pants or change into a procedure gown depending on access.
- 2
Quick exam first
I'll examine the hip, watch you move, and confirm the diagnosis we discussed. If anything has changed, we'll talk about it before we proceed.
- 3
Positioning
You'll lie on your back on the exam table. The skin over the front of your hip will be cleaned with sterile solution.
- 4
Ultrasound first look
I'll place the ultrasound probe on your skin to find the right window. The screen shows me the femoral head, the joint capsule, and the blood vessels we want to stay clear of. This takes 30 seconds.
- 5
Numbing the skin
I'll inject a small amount of local numbing medication into the skin and deeper tissue. Brief sting for a few seconds, then it goes numb.
- 6
The injection itself
Watching the screen the whole time, I guide a thin needle to the joint capsule. You'll see the needle on the screen too if you want — most patients find it reassuring. Once I confirm I'm in the right space, I deliver the medication. You may feel mild pressure or a brief stretch.
- 7
Walking out
I'll have you stand up, walk a few steps, and tell me how the joint feels. If the immediate relief is dramatic, that confirms the joint was the source. You can drive yourself home and resume normal light activity.
After
Recovery and what to watch for
Recovery from an office-based ultrasound injection is usually unremarkable. Most patients are back to their normal day within hours.
First few hours
The numbing medication may give you dramatic immediate relief. Enjoy it — it's diagnostic. Drive home, take it easy, no heavy lifting or pounding exercise for the rest of the day.
Hours 4–48
The numbing medication wears off and the steroid hasn't fully kicked in yet. Some patients have a 'flare' — temporary worsening of pain — in this window. Ice, Tylenol, normal anti-inflammatories. This is expected and self-resolves.
Days 3–7
The steroid starts working. Most patients notice meaningful improvement during this window. Resume normal activity, including PT if we agreed on it.
Weeks 2–6
Peak benefit. This is when most patients feel the best results. Use this window to do the strengthening work that produces durable relief.
When to call me right away
Severe new weakness in your arms or legs
If a limb feels significantly weaker than before — trouble lifting it, dragging a foot, dropping things — that needs attention now.
Loss of bladder or bowel control
Sudden trouble holding it or sudden trouble going. Rare, but a true emergency. Go to the ER, then call me.
Fever above 101°F (38.3°C)
A fever in the days after the procedure, especially with chills, can mean infection.
Spreading redness, warmth, or drainage at the injection site
Some bruising and tenderness is normal. Pus, increasing redness expanding outward, or yellow drainage is not.
Severe new pain that's worse than before
Brief soreness for a few days is expected. Sharp, severe new pain different from your usual is not.
For anything that worries you, call my office. I'd much rather hear from you and tell you it's fine than have you wait at home wondering. For loss of bladder/bowel control or anything that feels like a true emergency, go to the nearest ER — then call me.
The questions I get most
Frequently asked
Will I be put to sleep?
Why ultrasound and not X-ray?
Can I drive myself home?
How fast will I feel better?
How long does the relief last?
Can I have it again?
Will it hurt?
What if it doesn't work?
Have Questions?
If you'd like to learn more about your treatment options or have a question for Dr. Patibanda, reach out.
Contact Dr. Patibanda