Fluoroscopy-guided spine injection
Thoracic Epidural Steroid Injection
If you have mid-back pain or band-like nerve pain wrapping around your chest or upper abdomen, a thoracic epidural injection often helps. It's less common than cervical or lumbar, but for the right patient it can be the missing piece. Here's exactly what I'll do.
What I'm doing
Calming an irritated nerve in your mid-back
The thoracic spine is the long stretch in the middle, between your neck and your low back. The nerves there feed your chest wall and upper abdomen. When one of them is irritated — by a herniated disc, shingles aftermath (post-herpetic neuralgia), or a compression fracture — the pain often wraps around your trunk in a band.
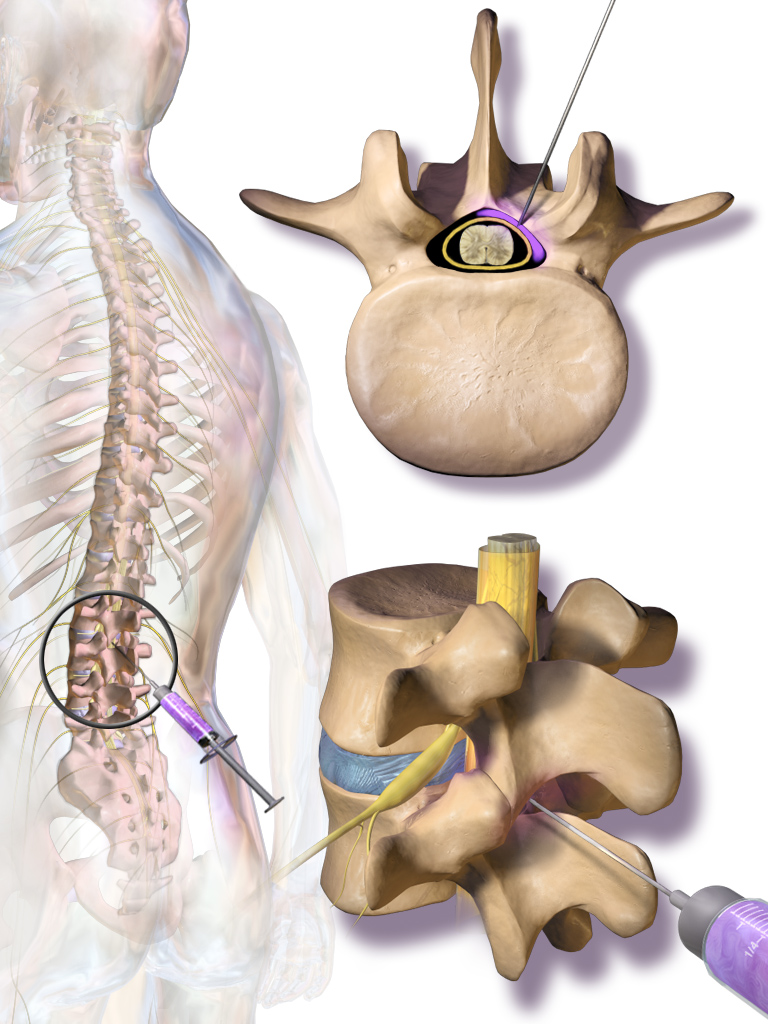
I deliver a small dose of anti-inflammatory medication into the thoracic epidural space — the cushion of fat just outside the sac holding your spinal cord. The medicine quiets the inflammation around the nerve and lets it heal.
The thoracic level is technically more demanding than the lumbar — the epidural space is narrower, the spinous processes angle steeply, and the spinal cord is right behind. I do every thoracic epidural under live X-ray with contrast confirmation. I will not advance the needle without seeing exactly where I am.
Two things this is especially useful for: post-herpetic neuralgia (chest or back pain lingering after shingles), and vertebral compression fracture painin the early healing phase. It's also the right tool when imaging points to a thoracic disc herniation as the source of band-like nerve pain.
Honest expectations
What this can do — and what it can't
What this can do for you
- Cuts the inflammation around the irritated thoracic nerve, often dropping band-like or radiating chest-wall pain enough that you can sleep and function.
- Particularly useful for post-herpetic neuralgia (post-shingles pain) and vertebral compression fracture pain.
- Targets the actual source of pain — not a body-wide painkiller.
- Minimally invasive — needle only, same-day discharge.
Risks I'll be honest about
Most are uncommon, and I take specific precautions at the thoracic level.
- Soreness in the mid-back for a day or two(common)
- Brief bump in blood sugar — important for diabetics(common in diabetics)
- Brief facial flushing or fluid retention(occasional)
- Headache that gets worse when sitting up (post-dural-puncture)(uncommon, treatable)
- Infection at the injection site(rare with sterile technique)
- Pneumothorax (rare lung injury) — the reason I use live X-ray(very rare)
- Spinal cord injury — vanishingly rare with image guidance(very rare)
Other options
Things we could try instead, or alongside
Antiviral / nerve pain medications
For post-herpetic neuralgia, gabapentin or pregabalin and topical lidocaine patches are first-line.
Where this fits: Always part of the picture for post-shingles pain — the injection is when those alone aren't enough.
Physical therapy + postural work
Mid-back strengthening and thoracic mobility work, especially for compression fracture recovery.
Where this fits: Almost always — usually as the long-term plan.
Vertebroplasty / kyphoplasty
If your mid-back pain is from a recent vertebral compression fracture, a different procedure (cement augmentation) can stabilize the fractured bone.
Where this fits: Acute compression fracture, severe pain, conservative care has failed in the first few weeks.
Intercostal nerve block
If the pain is more focal along one rib than truly mid-back, a peripheral nerve block on that intercostal nerve may be more direct.
Where this fits: Focal chest-wall pain after shingles, rib trauma, or surgery.
Anti-inflammatory medications
NSAIDs can help, especially for compression fracture pain.
Where this fits: When kidneys and stomach can tolerate them.
Before your visit
How to get ready
One thing I want you to know first
You will not be put to sleep for this.A lot of patients walk in expecting general anesthesia — that's not what happens here. If we're using conscious sedation (only at the surgery center, only in select cases), you'll get a relaxant through an IV that takes the edge off. You'll still be awake. You'll still be able to talk to me. You just won't be anxious. Most patients say it felt easier than they imagined.
Bring a driver
Eating and drinking before
Take your morning medications
Blood thinners — talk to me first
- • Aspirin (81 mg) — usually OK to continue. I'll tell you if I want it held.
- • Plavix (clopidogrel) — typically held 5–7 days before
- • Eliquis (apixaban) — typically held 24–48 hours before
- • Xarelto (rivaroxaban) — typically held 24–48 hours before
- • Pradaxa (dabigatran) — typically held 24–72 hours, depending on kidney function
- • Warfarin (Coumadin) — typically held until INR is below 1.5
- • Lovenox (enoxaparin) — typically held 12–24 hours
Tell me about your allergies
What to wear
The day of
Step by step, what actually happens
- 1
Arrival and check-in
You'll come in with your driver, finish paperwork, change into a gown, and a nurse will start an IV.
- 2
I see you before we start
I'll go over the plan, answer questions, and confirm consent.
- 3
Into the procedure room
You'll lie face down on the procedure table. The C-arm sits over your mid-back.
- 4
Numbing the skin
I'll inject local numbing medication. Brief sting, then it goes numb.
- 5
The injection itself
Using live X-ray, I guide the needle to the targeted level, inject contrast to confirm placement, then deliver the medication. 10–25 minutes.
- 6
Recovery
About 30 minutes — vitals, snack, walk before discharge.

After
Recovery and what to watch for
First 24 hours
Take it easy. Ice the mid-back if it's sore. The numbing may give you a few hours of immediate relief.
Days 1–3
Mild soreness is normal. Your usual pain may briefly come back before the steroid kicks in. Don't panic.
Days 3–7
The steroid starts working. Most patients notice meaningful improvement during this window.
Weeks 2–6
Peak benefit. Use this window for rehab and gradual return to activity.
When to call me right away
Severe new weakness in your arms or legs
If a limb feels significantly weaker than before — trouble lifting it, dragging a foot, dropping things — that needs attention now.
Loss of bladder or bowel control
Sudden trouble holding it or sudden trouble going. Rare, but a true emergency. Go to the ER, then call me.
Fever above 101°F (38.3°C)
A fever in the days after the procedure, especially with chills, can mean infection.
Spreading redness, warmth, or drainage at the injection site
Some bruising and tenderness is normal. Pus, increasing redness expanding outward, or yellow drainage is not.
Severe new pain that's worse than before
Brief soreness for a few days is expected. Sharp, severe new pain different from your usual is not.
Severe headache that gets worse when you sit or stand up
May be a post-dural-puncture headache. Treatable. Call me.
Sudden chest pain or shortness of breath
Thoracic-specific red flag (pneumothorax is rare but possible). Go to the ER, then call me.
For anything that worries you, call my office. I'd much rather hear from you and tell you it's fine than have you wait at home wondering. For loss of bladder/bowel control or anything that feels like a true emergency, go to the nearest ER — then call me.
The questions I get most
Frequently asked
Will I be put to sleep?
Is this riskier than a lumbar epidural?
Will it help my shingles pain?
How long does the relief last?
Can I drive myself home?
Will it hurt?
Have Questions?
If you'd like to learn more about your treatment options or have a question for Dr. Patibanda, reach out.
Contact Dr. Patibanda