Fluoroscopy-guided spine injection
Lumbar Epidural Steroid Injection
If you have shooting pain, numbness, or tingling running down a leg from your lower back, this is one of the most useful tools I have to help. Here's exactly what I'll do, why, and what to expect — in plain English, no medical jargon.
What I'm doing
Calming an angry nerve
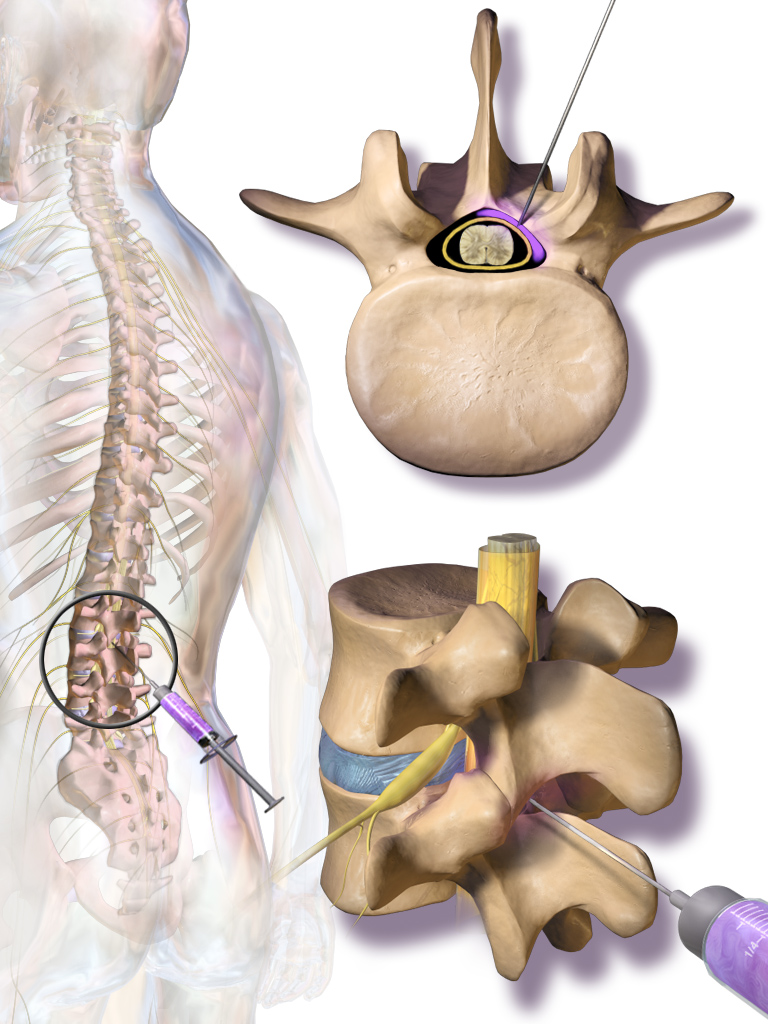
When a nerve in your lower back gets pinched or irritated — by a herniated disc, a bone spur, or a narrowed canal — it swells up. That swelling is what makes the pain shoot down your leg.
I deliver a small dose of anti-inflammatory medication — a steroid mixed with a local numbing medication — into the epidural space. That's the cushion of fat and tissue right outside the sac that holds your spinal cord and nerves. The medicine bathes the irritated nerve and quiets the inflammation down. The nerve gets a chance to heal. You get a chance to move again.
If you've heard the word epiduralin the context of childbirth, the location is similar but the goal is different. I'm not numbing you for surgery. I'm reducing inflammation that's been driving your pain.
Depending on what your imaging shows and where your pain is, I'll choose between an interlaminar approach (medication spreads broadly across the back of the spine) or a transforaminalapproach (medication is directed precisely at a single nerve root through the opening where it exits the spine). Both are safe. Both are effective. The right one depends on your case, and I'll explain my reasoning before we start.
Honest expectations
What this can do — and what it can't
I want you to walk in with the right picture. Most patients get real, meaningful relief. Not everyone does. I'll tell you the truth either way.
What this can do for you
- Cuts the inflammation around the irritated nerve, often dropping pain enough that you can move, sleep, and do physical therapy.
- Targets the actual source of your pain — not a generic painkiller fanning across your whole body.
- Minimally invasive — a needle, no incision, no stitches. You go home the same day.
- Often helps you avoid or delay back surgery.
- Decades of safety data behind it. One of the most studied procedures in pain medicine.
Risks I'll be honest about
Most are uncommon and most are short-lived.
- Soreness at the injection site for a day or two(common)
- A short bump in blood sugar — important if you have diabetes(common in diabetics)
- Brief facial flushing or fluid retention from the steroid(occasional)
- A headache that gets worse when you sit up — caused by a tiny membrane puncture(uncommon, treatable)
- Infection at the injection site(rare with sterile technique)
- Nerve injury(very rare)
- Allergic reaction to the steroid, contrast, or numbing medication(rare)
A word on the steroid itself
I usually limit you to no more than 3 lumbar epidural injections in the same area per year. Steroids are powerful, and over time they can affect surrounding bone and soft tissue. If you're needing them more often than that, we should be talking about a different approach — radiofrequency ablation, a longer-term plan with physical therapy, or something else. I'd rather solve the problem than chase it.
Other options
Things we could try instead, or alongside
An injection isn't the only path. Depending on your case, any of these may make more sense as the next move — and we'll talk about them honestly before we commit.
Physical therapy
Targeted strengthening of your core, hips, and lower back. The single most under-used tool in pain medicine.
Where this fits: Almost everyone benefits — often as the foundation that an injection just gets you back to.
Anti-inflammatory medications
Oral NSAIDs (ibuprofen, naproxen, meloxicam) or short oral steroid tapers can calm inflammation without a needle.
Where this fits: First-line for acute flares, when your kidneys and stomach can tolerate them.
Nerve pain medications
Gabapentin or duloxetine can quiet the kind of nerve pain that shoots down your leg.
Where this fits: When the pain is more nerve-type (burning, tingling, electric) than mechanical.
Radiofrequency ablation (RFA)
If the pain ends up being from your facet joints rather than a pinched nerve root, RFA gives 6–18 months of relief.
Where this fits: When diagnostic blocks confirm the facet joints are the source. Different problem, different tool.
Surgical consultation
If your imaging shows a problem that's likely structural — severe stenosis, instability, progressive weakness — surgery may be the right answer.
Where this fits: When conservative care has failed, when there's neurological loss, or when imaging clearly explains your symptoms.
Watchful waiting
A real and underrated option. Most disc herniations resorb on their own over weeks to months.
Where this fits: Mild symptoms, no red flags, and you can manage with rest and basic anti-inflammatories.
Before your visit
How to get ready
A few important things — please read all of them. Skipping any one of these can mean we have to cancel and reschedule, which I'd rather not do.
One thing I want you to know first
You will not be put to sleep for this.A lot of patients walk in expecting general anesthesia — that's not what happens here. If we're using conscious sedation (only at the surgery center, only in select cases), you'll get a relaxant through an IV that takes the edge off. You'll still be awake. You'll still be able to talk to me. You just won't be anxious. Most patients say it felt easier than they imagined.
Bring a driver
Eating and drinking before
Take your morning medications
Blood thinners — talk to me first
- • Aspirin (81 mg) — usually OK to continue. I'll tell you if I want it held.
- • Plavix (clopidogrel) — typically held 5–7 days before
- • Eliquis (apixaban) — typically held 24–48 hours before
- • Xarelto (rivaroxaban) — typically held 24–48 hours before
- • Pradaxa (dabigatran) — typically held 24–72 hours, depending on kidney function
- • Warfarin (Coumadin) — typically held until INR is below 1.5
- • Lovenox (enoxaparin) — typically held 12–24 hours
Tell me about your allergies
What to wear
The day of
Step by step, what actually happens
The whole appointment from check-in to walking out is usually 1.5–2 hours. The injection itself is much shorter — often under 5 minutes for a straightforward case.
- 1
Arrival and check-in
You'll come in with your driver, finish any remaining paperwork, change into a gown, and a nurse will start an IV.
- 2
I see you before we start
I'll come in, go over the plan again, answer any last questions, and confirm consent. This is the time to bring up any allergies, any medications you're not sure about, anything weighing on you.
- 3
Into the procedure room
You'll lie face down on the procedure table. The room has the C-arm X-ray and a monitor. Your back will be cleaned with sterile solution and draped.
- 4
Numbing the skin
I'll inject a local numbing medication into the skin and the deeper tissue. You'll feel a brief sting for a few seconds, then it goes numb.
- 5
The injection itself
Using live X-ray, I guide a thin needle to the right spot, inject a small amount of contrast dye to confirm the medication will spread correctly, then deliver the steroid and anesthetic. You may feel pressure or a brief reproduction of your usual pain — that's a good sign that I'm in the right place. Total time: most often under 5 minutes; up to 15–20 if your anatomy is complicated.
- 6
Recovery
We'll move you to recovery for about 30 minutes — vital signs, a snack, making sure your legs work normally before you stand up. Then your driver takes you home.

After
Recovery, activity, and what to watch for
Most patients are surprised how quickly they're back to normal life. Here's the realistic picture.
First 24 hours
Take it easy. Ice the injection area for 15–20 minutes a few times if it's sore. The numbing medication may give you a few hours of immediate relief — that's the local anesthetic, not the steroid yet. Your legs may feel heavy or warm. That fades.
Days 1–3
Mild soreness at the injection site is normal. Your usual pain may briefly come back or even feel slightly worse before the steroid kicks in. Don't panic. This is expected.
Days 3–7
The steroid starts working. Most patients notice meaningful improvement during this window. Resume light activity as you feel ready.
Weeks 2–6
Peak benefit. This is when most patients feel best. This is also when I want you in physical therapy if we agreed on it — the injection bought you a window to do the work.
When to call me right away
Severe new weakness in your arms or legs
If a limb feels significantly weaker than before — trouble lifting it, dragging a foot, dropping things — that needs attention now.
Loss of bladder or bowel control
Sudden trouble holding it or sudden trouble going. Rare, but a true emergency. Go to the ER, then call me.
Fever above 101°F (38.3°C)
A fever in the days after the procedure, especially with chills, can mean infection.
Spreading redness, warmth, or drainage at the injection site
Some bruising and tenderness is normal. Pus, increasing redness expanding outward, or yellow drainage is not.
Severe new pain that's worse than before
Brief soreness for a few days is expected. Sharp, severe new pain different from your usual is not.
Severe headache that gets worse when you sit or stand up
If a headache comes on a day or two after and is markedly worse upright than lying flat, that may be a post-dural-puncture headache. Treatable. Call me — don't tough it out.
For anything that worries you, call my office. I'd much rather hear from you and tell you it's fine than have you wait at home wondering. For loss of bladder/bowel control or anything that feels like a true emergency, go to the nearest ER — then call me.
The questions I get most
Frequently asked
Will I be put to sleep?
How fast will I feel better?
How long does the relief last?
Can I drive myself home?
Will it hurt?
What if it doesn't work?
Is this the same as back surgery?
Have Questions?
If you'd like to learn more about your treatment options or have a question for Dr. Patibanda, reach out.
Contact Dr. Patibanda