Fluoroscopy-guided spine procedure
Cervical Facet Radiofrequency Ablation
If your neck pain comes from the small joints in your cervical spine — not from a pinched nerve running down your arm — this is the procedure I reach for. Heat to quiet the tiny nerves carrying the pain signal. Months to over a year of relief.
What I'm doing
Quieting the pain pathway in your neck
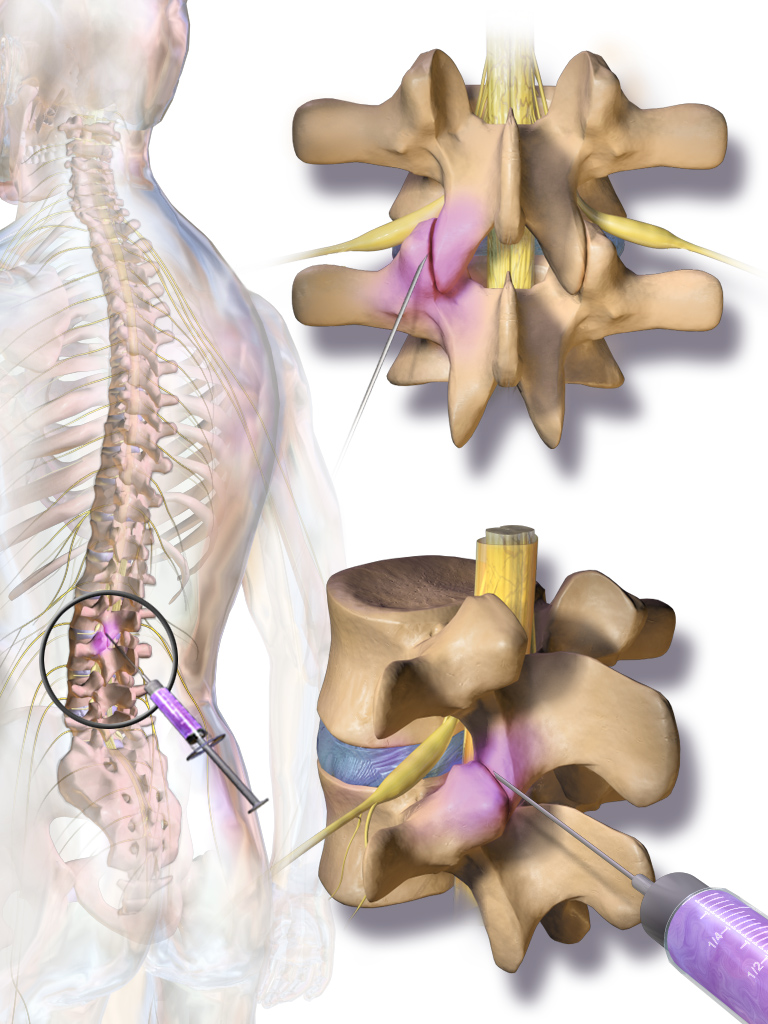
Your cervical spine has small joints — facet joints — at every level. They wear down with age, whiplash, and repetitive loading. When they hurt, the pain shows up as deep, axial neck pain that gets worse with extending or rotating your head. The pain travels through tiny nerves called medial branches.
Cervical facet RFA uses controlled heat to interrupt those medial branch nerves at the cervical levels. The joints stay. The arthritis stays. The pathway carrying the pain signal up to your brain is what changes.
Before I do an RFA, I almost always do diagnostic medial branch blocksfirst — usually two on separate days. I numb the same nerves with a temporary anesthetic. If the blocks give you significant relief, the facets are the source and RFA will likely help. If they don't, RFA isn't the right tool and we should look elsewhere.
The cervical level is technically more demanding than the lumbar — the medial branches sit very close to vertebral arteries and the spinal cord. I do every cervical RFA under live X-ray with sensory and motor testing before each treatment, never blind. Same caution I apply to cervical epidurals.
And I'll be straight with you: not everyone responds to RFA, even after positive diagnostic blocks. Most patients do — but a real fraction don't get the relief they hoped for. That's biology, not failure on either of our parts.
Honest expectations
What this can do — and what it can't
What this can do for you
- Long-lasting relief — typically 6 to 18 months from a single treatment.
- Often cuts or eliminates the need for daily neck pain medication.
- Lets you turn your head, sleep, and work without constant background pain.
- Minimally invasive — needles only, no incision, same-day discharge.
- Repeatable. The nerve regenerates over time, and we can treat again when it does.
Risks I'll be honest about
Most are manageable, and I take specific precautions at the cervical level.
- Soreness and muscle aching at the treatment sites for several days(common)
- Temporary numbness or skin sensitivity in the treated area(common, fades)
- Brief flare of usual pain in the first week(occasional)
- A small percentage of patients don't get the expected relief(uncommon but real)
- Infection at needle sites(rare)
- Vascular injury near the medial branch — the reason I use live X-ray and testing(very rare)
- Nerve injury affecting movement (medial branch is sensory only)(very rare)
Other options
Things we could try instead, or alongside
Repeat cervical facet injection
A direct steroid into the facet joint can give weeks to a few months of relief.
Where this fits: When you've responded well before and want a familiar, lower-commitment option.
Physical therapy + postural retraining
Deep cervical stabilizer training and postural work often reduces facet loading.
Where this fits: Always — usually as the long-term plan.
Cervical epidural injection
If your imaging or symptoms also suggest a pinched nerve (arm pain, numbness, tingling), an epidural targets a different problem.
Where this fits: When pain shoots down an arm — that's nerve-root, not facet.
Anti-inflammatory medications
NSAIDs (ibuprofen, naproxen, meloxicam) can dial down facet inflammation.
Where this fits: First-line, especially during a flare.
Surgical consultation
If imaging shows instability or severe stenosis that won't be fixed by quieting nerves, surgery may be the right move.
Where this fits: When conservative + interventional care has failed and imaging clearly explains the symptoms.
Before your visit
How to get ready
One thing I want you to know first
You will not be put to sleep for this.A lot of patients walk in expecting general anesthesia — that's not what happens here. If we're using conscious sedation (only at the surgery center, only in select cases), you'll get a relaxant through an IV that takes the edge off. You'll still be awake. You'll still be able to talk to me. You just won't be anxious. Most patients say it felt easier than they imagined.
Bring a driver
Eating and drinking before
Take your morning medications
Blood thinners — talk to me first
- • Aspirin (81 mg) — usually OK to continue. I'll tell you if I want it held.
- • Plavix (clopidogrel) — typically held 5–7 days before
- • Eliquis (apixaban) — typically held 24–48 hours before
- • Xarelto (rivaroxaban) — typically held 24–48 hours before
- • Pradaxa (dabigatran) — typically held 24–72 hours, depending on kidney function
- • Warfarin (Coumadin) — typically held until INR is below 1.5
- • Lovenox (enoxaparin) — typically held 12–24 hours
Tell me about your allergies
What to wear
The day of
Step by step, what actually happens
The whole appointment runs about 1.5–2 hours. The procedure itself takes 30–45 minutes since I'm treating multiple nerves at multiple levels.
- 1
Arrival and check-in
You'll come in with your driver, finish paperwork, change into a gown, and a nurse will start an IV.
- 2
I see you before we start
I'll go over the plan and which levels we're treating, answer questions, confirm consent.
- 3
Into the procedure room
You'll lie face down on the procedure table with your forehead supported. The C-arm sits over your neck, with a monitor beside it.
- 4
Numbing the skin
I'll inject local numbing medication at each treatment spot. Brief stinging, then it goes numb.
- 5
Positioning the probes
Using live X-ray, I guide thin RF probes to each medial branch nerve at the cervical levels we're treating. I test each placement first with a brief electrical pulse — sensory then motor — to confirm I'm at the right nerve and not too close to a major motor branch.
- 6
The treatment itself
Once each placement is verified, the probe heats the nerve to about 80°C for 60–90 seconds. You'll feel deep warmth and pressure, sometimes a brief reproduction of your usual neck pain. I treat both sides at the targeted levels.
- 7
Recovery
About 30 minutes in recovery — vitals, snack, walking around. Then your driver takes you home. You'll be sore.

After
The recovery you should plan for
Days 1–5: the sore phase
Expect deep aching at the treatment sites — like a sunburn buried inside your neck. Ice 15–20 minutes a few times a day. Your usual neck pain medication for breakthrough discomfort. Light walking is fine; avoid heavy lifting.
Week 1–2: the transition
Soreness fades gradually. Your usual pain may still be present — this is the in-between window when the nerves haven't fully quieted yet.
Weeks 2–4: real benefit shows up
This is when most patients notice the turning point. As treated nerves stop firing, neck mobility improves and the constant background pain quiets down. Resume normal activity. Restart physical therapy.
Months 1–18: sustained relief
Most patients enjoy 6 to 18 months of meaningful improvement. The nerves slowly regenerate over time — and when they do, we can repeat. Repeat RFAs usually work as well as the first.
When to call me right away
Severe new weakness in your arms or legs
If a limb feels significantly weaker than before — trouble lifting it, dragging a foot, dropping things — that needs attention now.
Loss of bladder or bowel control
Sudden trouble holding it or sudden trouble going. Rare, but a true emergency. Go to the ER, then call me.
Fever above 101°F (38.3°C)
A fever in the days after the procedure, especially with chills, can mean infection.
Spreading redness, warmth, or drainage at the injection site
Some bruising and tenderness is normal. Pus, increasing redness expanding outward, or yellow drainage is not.
Severe new pain that's worse than before
Brief soreness for a few days is expected. Sharp, severe new pain different from your usual is not.
Severe new arm weakness or trouble swallowing
Cervical-specific red flag. Rare, but a true emergency. Go to the ER, then call me.
For anything that worries you, call my office. I'd much rather hear from you and tell you it's fine than have you wait at home wondering. For loss of bladder/bowel control or anything that feels like a true emergency, go to the nearest ER — then call me.
The questions I get most
Frequently asked
Will I be put to sleep?
Why do you do the nerve blocks before the RFA?
Is cervical RFA riskier than lumbar RFA?
How quickly will I feel better?
How long does the relief last?
What if it doesn't work?
Can I have it more than once?
Can I drive myself home?
Have Questions?
If you'd like to learn more about your treatment options or have a question for Dr. Patibanda, reach out.
Contact Dr. Patibanda