If your back has been hurting for weeks or months, the first question I want to answer with you is a simple one: where is the pain coming from?
Most of the back pain I treat comes down to one of two things. A disc that is irritating a nerve, or arthritis of the small joints in the spine. Both are common. Both are treatable. But the right treatment is different for each — and getting it wrong wastes your time, your money, and sometimes your patience with the whole process. So before we treat anything, we figure out which one is driving the pain.
Here is how I think about it, in plain language.
Diagnosis
The two usual suspects
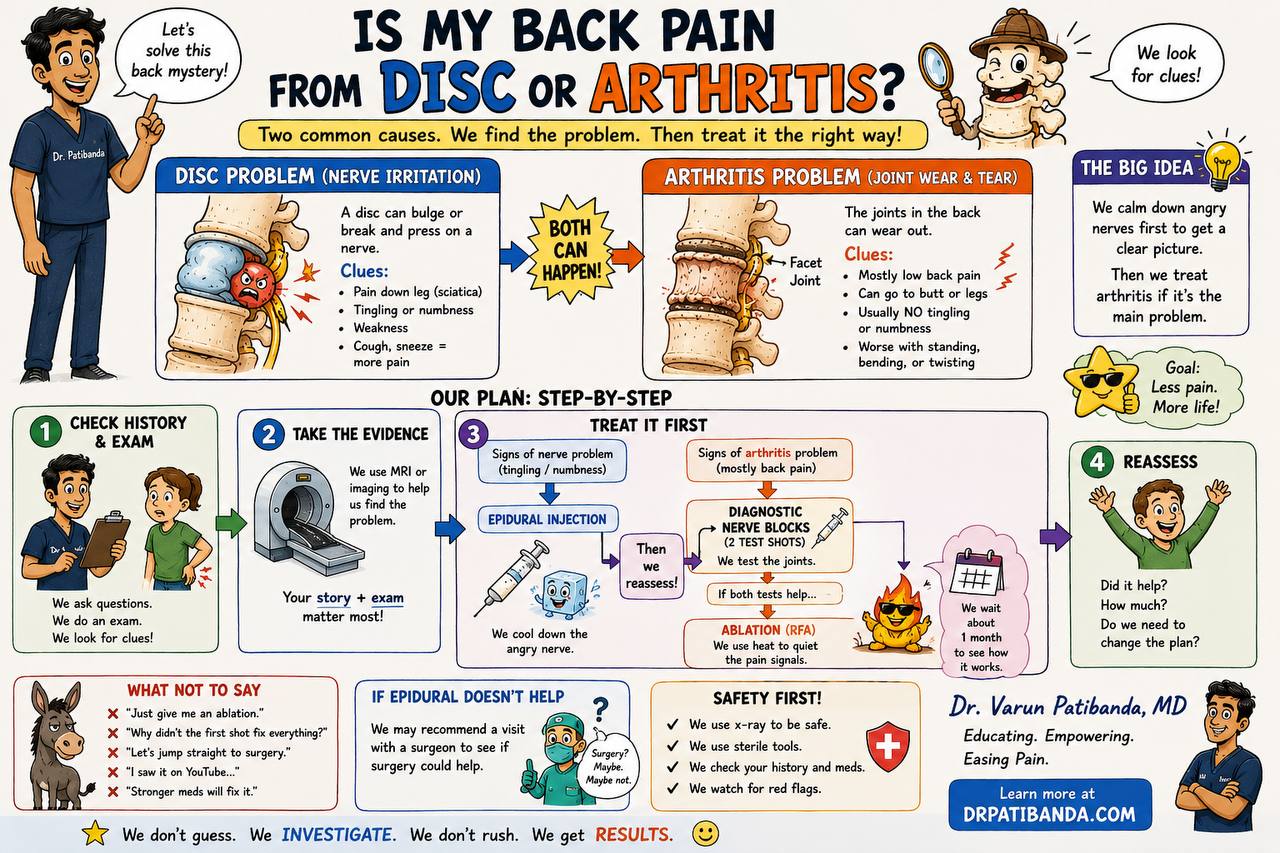
Disc problem (nerve irritation). Between each pair of bones in your spine sits a cushion called a disc. When a disc bulges or tears, it can press on one of the nerves that leaves your spine and travels down into your leg. When that happens, the pain doesn't stay in your back — it travels. It runs down the back of your thigh, sometimes all the way to your foot. You may notice tingling, numbness, or weakness in the leg or foot. Coughing, sneezing, or straining often makes the pain worse, because those movements briefly raise pressure inside the spine and on the nerve. This pattern is what most people call “sciatica.”
Arthritis problem (joint wear and tear). Your spine also has small joints in the back of it called facet joints. Like a knee or a hip, they can wear out over time. When facet arthritis is the problem, the pain stays mostly in your low back. It can spread into your buttock or the back of your thigh, but it usually does not run all the way down the leg, and you usually do not get tingling or numbness. It tends to get worse with standing, bending backward, or twisting — anything that loads those small joints — and better with sitting or leaning forward.
Both can happen at the same time. That is normal, especially over the age of fifty. My job is not to label everything you have on a scan — it is to figure out which one is driving the pain right now, because that is what we have to treat.
Workup
My plan, step by step
1. History and exam
I ask a lot of questions and put my hands on your back. Where exactly does it hurt? When did it start? What position makes it better or worse? Does it travel? Have you had it before?
You may notice I spend more time on the story than on the exam itself. That is intentional. Disc pain and facet pain behave differently in your daily life — when the pain wakes you up, what makes it ease, how it changes through the day — and those differences are usually the first real clue to the diagnosis. The story tells me which problem to look for; the exam tells me whether I am right.
In the exam itself, I am doing specific tests on purpose. Lifting your straight leg from the table loads the nerve roots and provokes pain that comes from a disc. Bending you backward or rotating your spine loads the facet joints and provokes pain that comes from arthritis. Checking your strength and reflexes tells me whether a nerve is being irritated enough to lose function — which changes how urgently we move. Each maneuver is asking a separate, narrow question. By the end I usually have a working diagnosis, and about 70 to 80 percent of the time I am already confident before any imaging is ordered.
2. Take the evidence
If we need it, I order an MRI or another image. Imaging is helpful, but only when it matches your story. Almost everyone over forty has something on an MRI — a bulge, a worn disc, a small bone spur. Those findings are common and most of them are silent. A scan is meaningful only when the picture lines up with what you are actually feeling.
3. Treat it first — and watch what happens
This is the part of the plan most patients haven't seen explained, so I want to slow down here.
If the picture looks like a nerve problem, I usually start with an epidural steroid injection. Under live X-ray guidance, I place a small dose of anti-inflammatory medication right next to the irritated nerve and the inflamed disc.
Here is what the steroid is actually doing. When a disc bulges, the pain is not only mechanical — it is also chemical. The disc material itself releases inflammatory proteins that irritate the nerve, and the nerve swells. A swollen nerve in a tight space hurts. The steroid reduces that inflammation, the nerve calms down, and the pain often eases enough that the underlying disc problem has time to heal on its own (which most discs do, slowly, over weeks to months). The injection itself takes about ten minutes. I use live X-ray — not blind anatomy — because the target is small, the nerves are close, and I want to see exactly where the medication is going before I deliver it.
Many patients feel meaningful relief within a week or two. Some patients need a second epidural a few weeks after the first, and occasionally a third. There is nothing wrong with needing more than one. A single injection is sometimes enough to break the inflammatory cycle, but more stubborn nerve irritation often needs the second dose to fully quiet down. For the patients an epidural does not fully fix, the partial relief still buys us a window to do physical therapy more effectively — which, long-term, is what actually keeps the pain from coming back.
If the picture looks like an arthritis problem, I do not jump straight to a “burning” procedure. Instead, I perform two short diagnostic nerve blocks on the small nerves (called medial branches) that carry signals from the facet joints. These are intentionally small test injections — their job is to answer a question, not to treat.
You may wonder why I do two rounds instead of one. The reason is honest and worth knowing.
A single block can give a misleading answer. Pain is a complicated signal, and the body responds to any injection — a small placebo effect, the local numbing of nearby tissue, the relief of finally doing something — for a few hours after the procedure. Studies have shown that if I rely on a single positive block, roughly one in three patients will get good relief from that test for reasons that have nothing to do with their facet joints. If I were to take those patients straight to radiofrequency ablation, a real procedure with a real recovery, a sizeable fraction of them would not benefit. They would have gone through a treatment for the wrong diagnosis.
A second block, performed on a separate day, with a different short-acting numbing medication, dramatically cuts that false-positive rate. If both injections give you clear, meaningful relief — typically defined as at least 80 percent improvement for the duration the medication is active — I can be confident the facet joints really are the source. At that point, RFA is the right next step. This is also why insurance — Medicare and most commercial plans — requires the two-block confirmation before authorizing the ablation. It is a real clinical safeguard, not a paperwork formality.
Once both tests confirm the diagnosis, I offer radiofrequency ablation (RFA) — a procedure that uses gentle heat to quiet those small nerves so they stop sending pain signals. RFA relief often lasts six months to a year or more, and the procedure can be repeated when the nerves grow back.
4. Reassess
About a month after a procedure I want to know: did it help? How much? Are you doing more of the things you stopped doing? Pain care is a moving target, and the plan should move with it. Sometimes we repeat what worked. Sometimes we change direction entirely. That is normal, and it is part of why we plan in steps instead of committing to one big swing.
What not to ask for
What I do not want you asking for
Patients sometimes come in with the answer already chosen — “just give me the ablation,” “let's skip to surgery,” “stronger pain meds will fix this,” “I saw something on YouTube.” I understand the urgency. Living with back pain is exhausting and you want it over with. But picking the procedure before we know the diagnosis is the most common way I see people end up with treatments that don't help them. The shortcut is the slow road. The careful workup is what actually gets you back to your life.
Safety
Safety, always
Every spine procedure I do is done under live X-ray guidance, with sterile technique, after a careful review of your medical history and medications — especially blood thinners and any implanted devices like a pacemaker. I am watching for red flags throughout — fever, new weakness, loss of bladder or bowel control — and if any of those appear, the plan changes immediately. If your case looks like one that would benefit from a spine surgeon's opinion, I will tell you that directly, and I will help you get there.
The bottom line
We don't guess. We investigate. We don't rush. We get results. That is the whole job.
Written by Dr. Varun Patibanda, M.D., D.A.B.P.M. Educational only — talk with your doctor about your specific case.